ADENOMATOID TUMOUR OF THE FALLOPIAN TUBE
Cussuma M Chodankar**,
Urmi Chakravarty*, Anjali V Dhurde**,
CP Shroff***
***Professor and Head; **Associate Professor; *Lecturer,
Department of Pathology, LTMMC and LTMGH, Mumbai 400 022.
Primary tubal neoplasms are rare
and are usually only recognised at surgery or on pathological examination
of the excised specimen. In contrast to malignant benign tumours of the
fallopian tube are rare. The most frequent of these is the adenomatoid
tumour.1 In most cases this tumour is an incidental finding. We present
a case where this tumour was found incidentally in the tubectomy specimen
of a 30 year old woman.
INTRODUCTION
The term adenomatoid tumour
was first proposed by Golden and Ash. [2] It is a rare
benign epithelial lesion with distinct morphology. Confined almost exclusively
to the genital sphere it is considered as a particular form of mesothelioma.
The benign adenomatoid tumour is now viewed as part of a spectrum of non-neoplastic
and neoplastic lesions of the highly reactive mesothelium. [3]
In most cases the tumour is an incidental finding as was in our case.
CASE REPORT
A thirty year old woman, gravida
2 and para 1, underwent an elective caesarean section for post datism.
Bilateral tubectomy was performed at the time of surgery as a family planning
procedure. Resected segments of both tubes were sent for routine histopathology
examination.
Pathological examination
Gross examination of the left
tubal segment revealed a well circumscribed, non-encapsulated firm, round
nodule 1.5 cm in diameter lying, beneath the serosa and causing narrowing
of the tubal lumen. Cut surface was smooth, homogeneous and glistening,
greyish white in colour (Fig. 1). Microscopic examination showed closely
packed adenoid, canalicular macrocystic and angiomatoid structures lined
by a low cuboidal non-mitotic epithelium. Stroma was sparsely cellular
(Figs. 2 and 3).
 |
| Fig 1 : Gross specimen of the left fallopian tube segment showing a well circumscribed non-encapsulated firm, round nodule causing narrowing of the tubal lumen. |
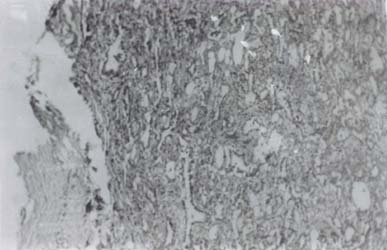 |
| Fig 2: Low magnification showing flattening of fallopian tube and closely packed adenoid, canalicular, macrocystic and angiomatoid structures(100 x) |
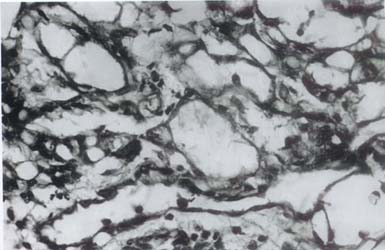 |
| Fig 3 : Higher manification showing closely packed adenoid canalicular and macrocystic structures lined by a low cuboidal, non-mitotic epithelium |
DISCUSSION
Although most reported examples
of adenomatoid tumours are in the male genital tract, in female patients
they occur in the fallopian tube and uterus with an equal frequency. In
the tube the tumour may be confined to the endosalpinx or more often in
the perisalpinx. Their size ranges from 1 mm to 3 cm. [4]
Ultrastructurally these tumours show features of normal peritoneal mesothelium and hence at present these tumours are considered to represent a localised benign form of mesothelioma. [5]
The tubal adenomatoid tumour is always asymptomatic and has no effect on tubal function.
REFERENCES
1. Haines, Taylor. Obstetrical and Gynaecological Pathology. Churchill Livingstone. 4th Edition. 1995; I : 639-40.
2. Golden A, Ash JE. Adenomatoid tumours of genital tract. Am J Path 1945; 21 : 63-79.
3. Bolen JW, Hammar SP, Macnutt MA. Reactive and neoplastic serosal tissue : a light microscopic, ultrastructural and immunohistochemical study. Am J Surg Pathol 1986; 10 : 34-47.
4. Honore LH, OHara KE. Adenomatoid tumour of the fimbrial endosalpinx a report of two cases with discussion of histogenesis. Eur J Ostet Gynecol Reprod Biol 1979b; 53 : 335-39.
5. Taxy
B, Battifora H, Oyasu R. Adenomatoid tumours a light microscopic, histochemical
and ultrastructural study. Cancer 1974; 34 : 306-16.